Choosing a hip surgeon is one of the most consequential medical decisions you will ever make. The surgeon you select determines the technique used, the implant chosen, where you undergo surgery, how quickly you recover, and ultimately whether your hip pain becomes a memory or a lingering problem.
For patients in Englewood, Bergen County, and the surrounding communities of northern New Jersey, the good news is that access to genuinely elite, subspecialty hip care is available locally, without crossing into Manhattan. The challenge is knowing how to evaluate your options clearly, and how to separate real expertise from marketing.
This guide gives you seven concrete criteria to apply when choosing your hip surgeon. Each one reflects what the research shows and what decades of clinical experience confirm. Use this as a framework for your consultations, your questions, and your final decision.
1. Subspecialty Focus: Is Hip Surgery Their Primary Work or One of Many Things They Do?
This is the single most important question to ask, and the one most patients forget to ask at all. A surgeon who dedicates their practice primarily, or exclusively, to hip conditions will have seen more anatomical variations, performed more procedures, navigated more complex cases, and developed more refined protocols than a surgeon for whom hip replacement is one part of a general workload. They are also more likely to be current on the latest advances in technique, implant design, and perioperative care.
2. Surgical Volume: How Many Hip Replacements Does Your Surgeon Perform Each Year?
Volume is the variable that surgical outcome data returns to repeatedly, and the evidence is clear: higher-volume surgeons produce better results.
A study examining data from more than 20,000 surgeries found that more experienced surgeons were half as likely to need to perform a revision (repeat) surgery in the first six months. Revision surgery was required 0.7% of the time when performed by surgeons doing more than 50 hip replacements per year, compared to 1.3% for surgeons doing between 6 and 25 per year.
Fifty procedures per year is a threshold many researchers use as a marker for meaningful experience. But context matters. A surgeon performing 50 hip replacements annually while also doing knee, shoulder, and spine surgery is a different clinical proposition than a surgeon performing 200 or more hip procedures annually as their primary focus.
Do not hesitate to ask a prospective surgeon how many hip replacements they perform each year, and specifically how many using the technique they are recommending for you. A confident, experienced surgeon will answer that question directly. Evasiveness or vagueness about surgical volume is itself informative.
3. Surgical Approach: Do They Offer the Most Advanced Technique Available — and Are They Truly Expert in It?
Not all hip replacement techniques are equal, and not all surgeons who claim to perform minimally invasive hip replacement are equally skilled in doing so.
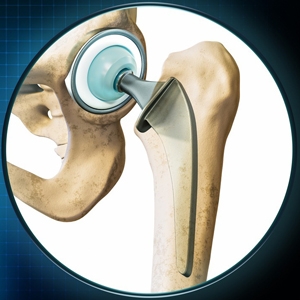
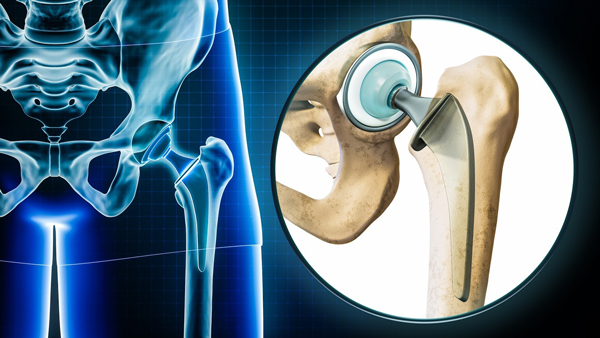
The Direct Anterior Approach Total Hip Replacement is the most tissue-preserving surgical technique currently available for hip replacement. It accesses the hip joint through a natural interval between muscles, rather than cutting through them. The major stabilizing muscles of the hip remain intact, which is why patients experience less postoperative pain, walk sooner, and recover faster than with traditional posterior or lateral approaches.
However, the anterior approach has a documented learning curve. Surgical volume directly correlates with outcomes in hip replacement, and this is especially true for the anterior approach, which requires specialized equipment, precise intraoperative positioning, and technique refinements that only accumulate through high case volume.
A surgeon who performs the anterior approach occasionally, or who recently adopted it after training in conventional posterior technique, cannot offer the same consistency and safety profile as one who has built an entire practice around it.
Before committing to a surgeon, ask: how many anterior approach hip replacements have you performed specifically? When did you adopt this technique? What is your dislocation rate and revision rate with this approach?
Dr. Davidovitch was the first surgeon in New York City to perform the Direct Anterior Approach Total Hip Replacement and have since completed more than 5,000 of these procedures. That level of specific anterior approach experience is not common, even among busy orthopedic practices.
4. Technology: Does Your Surgeon Have Access to, and Are They Certified in, the Latest Tools?
Advanced surgical technology does not substitute for surgical skill and experience. But in the hands of a high-volume, fellowship-trained specialist, the right technology adds a meaningful additional layer of precision.
The two technologies that represent the current standard of care in anterior hip replacement are:
Mako SmartRobotics™ The Mako system uses CT-based 3D modeling of the patient's unique anatomy to create a patient-specific preoperative surgical plan. During surgery, AccuStop™ haptic technology provides real-time guidance that keeps bone preparation and implant placement precisely within planned parameters. Research consistently demonstrates improved acetabular cup positioning accuracy and reduced dislocation rates with Mako-assisted technique compared to conventional manual surgery.
RotexTable® by Condor The anterior approach requires a specialized orthopedic table to allow controlled positioning of the operative leg throughout the procedure. The RotexTable, which Dr. Davidovitch co-designed based on more than 5,000 anterior approach cases, is the only fully automated orthopedic table of its kind. It is operated entirely by the surgeon, eliminating the manual positioning variability that exists with conventional traction tables.
When evaluating a hip surgeon, ask whether they use robotic assistance, which system they use, and whether they are certified in its use. Also ask whether they have access to a specialized table designed for the anterior approach. These are not trivial questions, the answers tell you a great deal about the seriousness and sophistication of the surgical environment.
5. Hospital and Facility Affiliation: Where Will Your Surgery Actually Be Performed?
The quality of your surgical outcome is not solely determined by your surgeon. The facility where your surgery is performed, the nursing staff, the anesthesia team, the post-anesthesia care unit, the implant inventory, the infection control protocols, all contribute to your result and your safety.
Hospital credentialing committees thoroughly review surgeon qualifications before granting privileges, providing an additional layer of quality assurance. A surgeon's hospital affiliation is therefore a proxy for their professional standing as well as an indicator of the clinical environment your care will occur in.
Ask any surgeon you are evaluating: where is my surgery performed? Is the facility accredited? Does it have the technology and staff experience specific to the procedure you are recommending?
6. Fellowship Training and Academic Standing: What Did Your Surgeon Do After Residency?
Orthopedic residency provides broad training across the full scope of musculoskeletal surgery. What a surgeon does after residency, specifically, whether they pursued additional subspecialty fellowship training and in what, is a meaningful differentiator.
Fellowship training specifically in joint replacement or adult reconstruction provides focused expertise in hip replacement techniques, implant selection, and complex cases beyond what orthopedic residency alone provides.
Beyond fellowship, academic standing, including hospital appointments, professorships, research publications, and membership in peer-reviewed professional societies, signals a surgeon who is held accountable to the highest professional standards and who contributes to advancing the field rather than simply practicing within it.
Dr. Davidovitch’s training includes subspecialty fellowship training in Orthopedic Trauma and Hip and Pelvis Reconstruction at Harvard Medical School, an AO International Fellowship in Computer Navigated Surgery at Hadassah Medical Center in Jerusalem, and a residency at NYU Langone's Hospital for Joint Diseases where he was awarded the Frauenthal Award for Excellence in Clinical Research. He currently hold the Julia Koch Endowed Professorship in Orthopedic Surgery at NYU Grossman School of Medicine, am elected to the American Hip Society, and have published more than 113 peer-reviewed papers.
These credentials are not listed for self-promotion. They are listed because they represent the kind of verifiable, independently evaluated markers of expertise that distinguish serious subspecialists from generalists, and they are the kinds of things you should be looking for when evaluating any hip surgeon.
7. Communication, Transparency, and Patient-Centered Care: Does This Surgeon Actually Listen?
Every criterion above is measurable and verifiable. This last one is harder to quantify but equally important to the experience of your care.
The best hip surgeon for you is not just the one with the most impressive credentials, it is the one whose credentials are strong and who communicates honestly, explains your options clearly, answers your questions without rushing you, and demonstrates a genuine commitment to your individual goals and circumstances.
Understanding individual expectations can lead to greater post-surgical patient satisfaction. A surgeon who takes the time to understand what you want from hip surgery, whether that is getting back to distance running, traveling without pain, keeping up with your grandchildren, or simply sleeping through the night, is a surgeon who can calibrate your care and set realistic, individualized expectations.
In your consultation, pay attention to how questions are handled. Are they addressed directly and completely, or deflected? Does the surgeon acknowledge uncertainty where it exists, or project false confidence? Is conservative management discussed honestly before surgery is recommended, or is the path to the operating room assumed from the start?
Bringing It All Together: What to Ask at Your Consultation
Use these seven criteria to structure the questions you ask at your surgical consultation. Here is a practical checklist:
- On focus and volume: What percentage of your practice is hip surgery? How many hip replacements do you perform per year? How many specifically using the approach you are recommending?
- On technique and technology: Do you perform the direct anterior approach? How many have you done? Do you use robotic assistance? Which system, and are you certified? What surgical table do you use?
- On facility: Where will my surgery be performed? Is it accredited? What is the facility's experience with anterior approach hip replacement specifically?
- On training: Where did you complete fellowship training? In what subspecialty? Are you board-certified in orthopedic surgery?
- On outcomes: What is your dislocation rate? What is your revision rate within the first year? What percentage of your appropriate patients go home the same day?
- On communication: What are all my options, including non-surgical? What recovery timeline should I realistically expect? What would make you advise against surgery in my case?
Why Patients Choose OrthoEnglewood and Dr. Roy I. Davidovitch, MD
For patients in Englewood, Fort Lee, Teaneck, Hackensack, Paramus, and throughout Bergen County, OrthoEnglewood brings the same level of subspecialty hip expertise available at the most advanced orthopedic centers in Manhattan, without the commute, the parking, or the impersonal experience of a large institutional practice.
Dr. Davidovitch’s practice at OrthoEnglewood offers:
- Exclusive subspecialty focus on all hip conditions in adolescents and adults
- Direct Anterior Approach Total Hip Replacement with over 5,000 procedures completed
- Mako SmartRobotics™ certified robotic-assisted hip replacement
- The RotexTable® by Condor, co-designed by Dr. Davidovitch for anterior approach surgery
- Same-day discharge (outpatient) hip replacement for appropriate candidates
- Full-spectrum hip preservation, including hip arthroscopy, labrum repair, PAO for dysplasia, and treatment of avascular necrosis
Ready to Schedule a Consultation?
If you are experiencing hip pain that is limiting your daily life, the first step is a thorough evaluation, not a commitment to surgery. A consultation gives you the information you need to make the right decision for your health, your recovery, and your life.
To schedule an appointment with Dr. Roy I. Davidovitch, MD at OrthoEnglewood, contact our office at 34 S Dean Street, Suite 202, Englewood, NJ 07631, or request an appointment online at anteriorapproachhipreplacementnyc.com.
Serving patients throughout Bergen County, including Englewood, Fort Lee, Teaneck, Hackensack, Paramus, Ridgewood, Cliffside Park, and surrounding northern New Jersey communities.
Reference Links:
About Dr. Roy I. Davidovitch, MD
Dr. Roy I. Davidovitch is a world-renowned orthopedic surgeon based in New York City, recognized as a leading authority in hip reconstruction and preservation. As the Director of the NYU Langone Hip Center and the Julia Koch Associate Professor of Orthopedic Surgery, he has dedicated his career to advancing the field of minimally invasive surgery. He holds the distinction of being the first surgeon in New York City to perform the Direct Anterior Approach total hip replacement, a milestone that has redefined the standard of care for patients seeking rapid recovery and muscle-sparing techniques.
With a clinical track record that ranks among the best in the nation, Dr. Davidovitch has performed over 10,000 hip procedures, including more than 6,000 Direct Anterior total hip replacements and over 2,000 outpatient procedures. His commitment to patient safety is evidenced by a remarkably low complication profile, maintaining less than a 0.1% risk for both infection and dislocation. By combining academic leadership with high-volume surgical expertise, Dr. Davidovitch provides patients in Manhattan and Princeton, NJ, with a path to long-term pain relief and a swift return to an active lifestyle.